ED Referral Algorithm for GPs
Erectile dysfunction (ED) is common in general practice and is frequently multifactorial (vascular, metabolic, medication-related and psychogenic components often coexist).¹ Importantly, ED can be a cardiovascular (CV) risk marker, so assessment should routinely include CV risk review rather than focusing only on sexual function.²–⁴
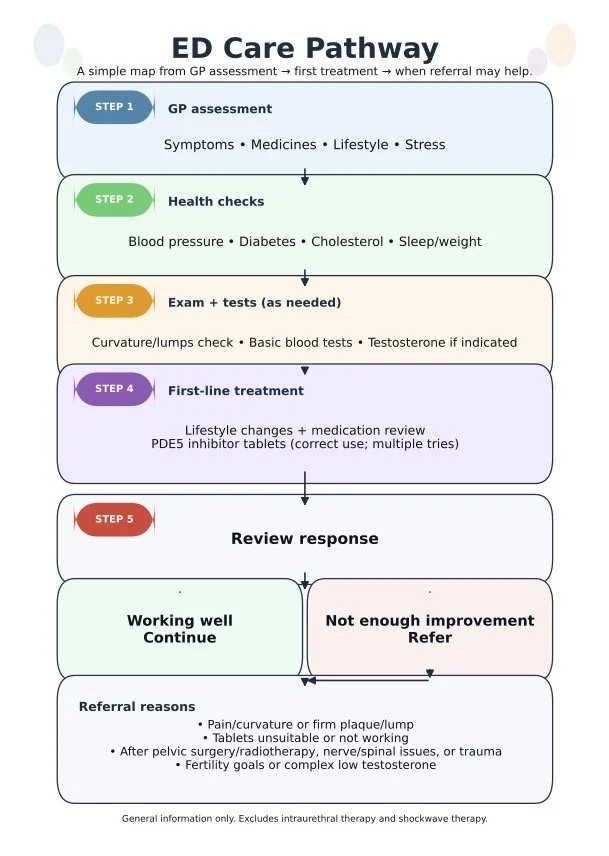
Quick ED referral algorithm
Step 1 — Confirm ED and screen for urgency
Clarify onset (sudden vs gradual), severity, morning/nocturnal erections, libido, ejaculation, relationship context, pelvic surgery/radiotherapy, trauma, alcohol/substances, and medication list (e.g., SSRIs, antihypertensives, opioids).¹–³
Urgent escalation if red flags (e.g., priapism).²
Step 2 — CV and metabolic risk check
Assess BP, diabetes risk (HbA1c/fasting glucose), lipids, smoking, obesity/OSA symptoms, and exercise tolerance; optimise risk factors in parallel with ED treatment.¹–⁴
Step 3 — Focused exam + baseline investigations
Genital exam for plaques/curvature (Peyronie’s) and testicular exam where relevant.²
Baseline bloods commonly include glucose/HbA1c, lipids, renal function.¹ Consider morning total testosterone when low libido, reduced morning erections, infertility, or symptoms of hypogonadism; if low, confirm and extend endocrine work-up as indicated.¹–³
Step 4 — First-line GP management
Lifestyle and risk-factor optimisation plus medication review.¹
Trial a PDE5 inhibitor with clear instructions and dose optimisation; inadequate education/under-dosing is a common reason for non-response.¹–³
Step 5 — Reassess and decide: continue vs refer
Continue if effective and tolerated.¹–³
Refer to urology/andrology when specialist input is likely to change management:
When to refer
Penile pain, curvature, palpable plaque, or deformity (suspected Peyronie’s).²
Failure of an optimised PDE5 inhibitor trial (correct use + adequate dosing + multiple attempts + comorbidity optimisation).¹–³
Post-pelvic surgery/radiotherapy ED, pelvic trauma, spinal cord injury, significant neurological disease.²³
Complex hypogonadism/endocrine concerns or fertility goals requiring coordinated assessment.²⁴
Patient preference for specialist-supported options such as vacuum device coaching, intracavernosal injection therapy, or penile prosthesis counselling.²³
What to include in your referral
Duration/severity, comorbidities/CV risk factors, medication trial details (drug/dose/attempts), relevant exam findings (plaques/curvature), baseline bloods (incl. testosterone if done), and fertility goals.²³
References
Lowy M, Ramanathan V. Erectile dysfunction: causes, assessment and management options. Aust Prescr.2022;45:159-161.
Burnett AL, Nehra A, Breau RH, et al. Erectile Dysfunction: AUA Guideline. J Urol. 2018;200(3):633-641.
European Association of Urology. EAU Guidelines on Sexual and Reproductive Health: Management of Erectile Dysfunction. EAU; 2024–2025 update.
Köhler TS, et al. Princeton IV Consensus Recommendations (ED and cardiovascular risk). J Sex Med. 2024.